
Figure 1: Primary Mass (11.5x12.5x2.8cm)
Granular cell tumors (GCT) are a rare soft tissue neoplasm of Schwann cell origin. This form of tumor is generally benign (0.5-2% malignant) and in these cases, involvement of the skin and deeper structures are not common, presenting usually as a solitary, slow-growing, painless mass (McGuire et al. 2014). This case report presents a 43-year-old woman with multiple benign slow growing masses on the back for 15 years, later biopsied to reveal benign granular cell tumor. Wide local excision of 2 masses and placement of wound VAC was performed by plastic surgery team with primary specimen measuring 11.5 x 12.5 x 2.5cm with skin and deep structure involvement, and a smaller mass measuring 6 x 3.1 & 5 x 2.1cm. Split-thickness skin graft was performed a week after confirmation from pathology on its benign nature. This case highlights an abnormal presentation of benign GCT due to size, skin and deep structure involvement, multiple lesions and appropriate management.
Granular cell tumors, also less commonly known as Abrikossoff tumors, are a rare soft tissue neoplasm consisting of only 0.5% of all soft cell tumors (Battistella et al. 2014). GCT is believed to be of neural origin and is characterized by large polyhedral cells containing eosinophilic cytoplasm and immunohistologically positive for S-100 and CD68 (Gündüz, 2016). These forms of tumor are generally benign (0.5-2% malignant) and are rarely multifocal, affecting age ranges of 30-50 years (Goel, 2013). In benign cases, involvement of the skin and deeper structures are not common. GCT tends to affect African-Americans more than whites, and are more likely to affect females 2x more than males (Fragulidis, 2011). These generally solitary, slow growing neoplasms are mainly found on the tongue, oral cavity, skin, and rarely in internal organs. Its malignant form tends to have deeper tissue invasion, large size recorded up to 15 cm, and rapid growth, with poor prognosis (McGuire, 2014).
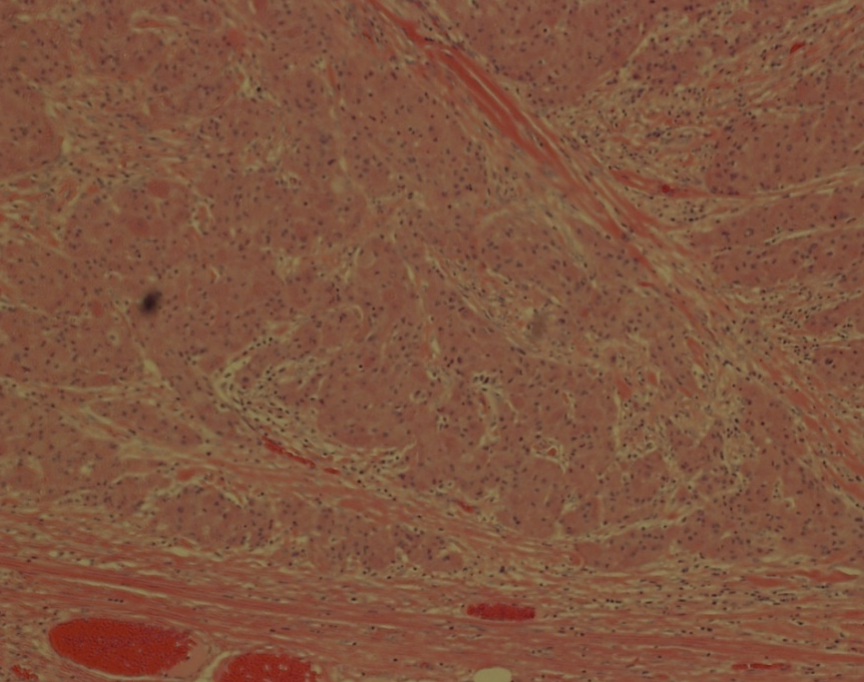
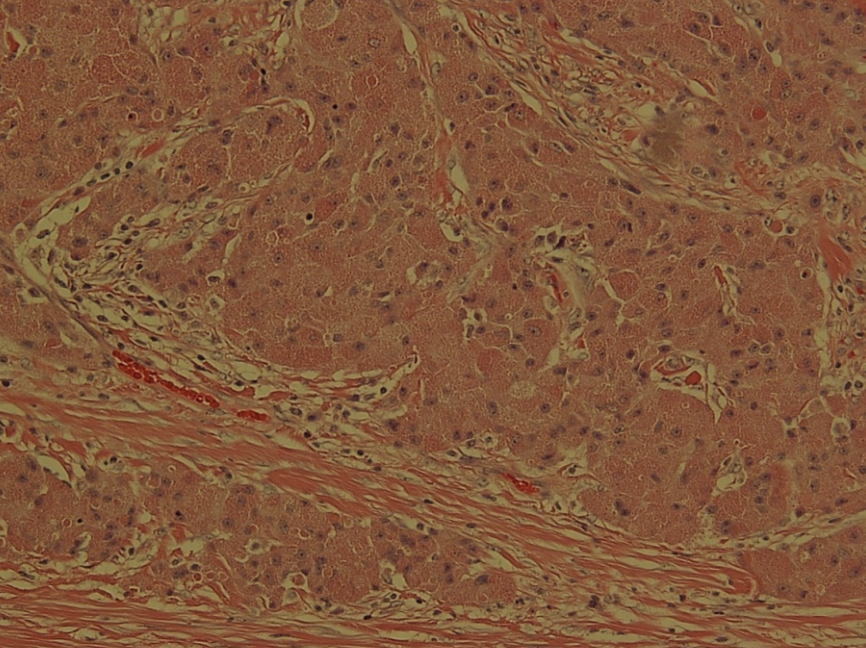
Granular cell tumor was initially believed to be of myoblastic origin for a long time due to similarities in appearance to skeletal cell tumors, however recent literature seems to point it of neural crest cell origin as demonstrated by S-100, CD68, SOX10 and peripheral nerve myelin protein positivity. These lesions tend to appear as large polygonal cells, small nuclei, and granular cytoplasm (Gayen et al., 2015). Upon histology, these cells are commonly separated by bands of collagen and fibrinous material. Cytoplasm granularity is due to large lysosomes which are filled with various cellular debris such as myelin proteins, mitochondria and rough endoplasmic reticulum fragments (Fragulidis, 2011).
Typical granular cell tumor presentations are during the ages of 30-40, with higher incidence in African-American females. A large majority of these lesions are benign, solitary, slow-growing, asymptomatic, firm nodule from 0.5 to 3.0 cm diameters. Prognosis of GCT tends to be very good after surgery with very few (2%) of GCT resulting in malignancy (Singh et al. 2015). Malignant GCT present as recurrent, fast growing, large lesions, lymph node involvement that have poor prognosis due to metastasis. Malignant GCT are characterized with necrosis, increased mitotic activity and increased nuclear to cytoplasm ratio with pleomorphism. Invasion to deep structures, vascular invasion, or involvement of skin are much more common in malignant GCT, however can happen in some cases of benign GCT (Battistella et al. 2013). In a large majority of benign GCT, excision is curative. In aggressive malignant forms, radiotherapy has seen some success in other forms of GCT, but prognosis remains poor and wide local excision remains gold standard in treatment (Gündüz, 2016).
In present literature, there are multiple cases presenting these lesions in different locations and various sizes. However, in this case, we present an unusual presentation of multiple benign, large GCT masses in a 43-year-old woman located on the back, with a large primary mass(11.5 x 12.5 x 2.5cm) with skin and deep structure involvement, and a smaller more typical GCT lesion on the back; uncommon in present literature for benign presentation.
The patient is a 43-year-old African-American female with complaints of a 15-year history of an enlarging mass on her right back. She denied any fever, chills, change of color or discharge, but described that within a year, the mass had progressively increased in size accompanied with pain and pruritus. The patient described pain when leaning on the lesion. Previous CAT scan had shown a 4x6cm mass but upon clinical examination 2 years later, revealed an 8x8 cm subcutaneous mass on the right mid-paramedial back as well as a secondary soft tissue non-characterized mass at her lower right paramedial back. FNA biopsy was performed, and histopathology revealed subcutaneous proliferation of cells between strands of dense fibrous tissue. Cells were medium in size and eosinophilic and granular cytoplasm. Nuclei were relatively small and uniform. Immunohistochemical staining revealed CD68 and S100, but negative MART1 expression; confirming diagnosis of GCT. Due to lesion's extensive attachment to the skin, patient was referred to the plastic surgeon for reconstruction. MRI revealed primary mass involvement of the paraspinous musculature. Secondary mass on the lower right side of the back showed non-adherence to the skin, but extensive attachment to the underlying fascia and musculature.
Excision of the primary mass was deep into the back fascia and some of the latissimus and paraspinous musculature due to lesion fixation. A separate incision was made at the lower back for the secondary lesion, in which the mass with some paraspinous musculature was excised. Final surgical pathology was 11.5 x 12.5 x 2.8cm (Figure 1) for the primary mass on the upper back and 6 x 3.1 & 5 x 2.1 cm (Figure 2) for the smaller secondary mass at the lower back. Both lesions were sent to the pathology lab with additional deep tissue to confirm diagnosis.

The secondary lesion was closed in layers of Monocryl sutures (8.3cm), while the primary lesion was installed a wound VAC pending pathology results due to size of lesion and reconstruction modality determination. Pathology results were negative for malignancy and invasion of surrounding tissue, and STSG reconstruction was done with Prevena wound VAC placement with no complications. Patient was sent home same day with no complications.
The patient of this case review was a 43-year-old African-American female with a 15-year history of an enlarging mass on her right middle back. She denied any fever, chills, change of color or discharge. Initially, the patient suspected the mass was a lipoma with its initially mobility and no other accompanying symptoms. However, within the past year, the mass rapidly expanded with pain and pruritus described "under the skin". The mass was noted to be especially tender on palpation and rubbing of the overlying skin. Our patient was in distress with complaints that the mass had impacted her life and made putting on clothing difficult. Upon ultrasound imaging revealed 8x8cm solid mass with signs of infiltration into the latissimus and paraspinous musculature. Further exploration in the OR revealed smaller secondary masses; unusual for benign GCT. Despite the abnormal presentation of GCT, the decision was made for wide excision of the mass with hopes that the tumor had not extensively infiltrated the muscle and that the tumor remained proximal to the skin.
Based on current literature, wide base excision would have been the gold standard therapy, however there was initial worry of the extent of muscle invasion underneath which would have altered the decision with fears of damaging the muscles. Fortunately, the mass had not reached into the deep back muscles and minimal musculature removal was required. If lesion had infiltrated past the deep fascia with extensive muscle involvement, consideration for radiotherapy/chemotherapy would be considered to reduce tumor size.
Due to the large size of the mass, consideration was taken into account into reconstructive options for the patient. A wound Vac was placed temporarily, and a future reconstructive surgery was scheduled for potential STSG for the patient. An additional smaller mass was also removed on the lower right back with minimal infiltration into the paraspinous muscle. Due to its small size, wound Vac was not needed and was promptly closed with stitches. The wide excision removal was an overlying success with the patient having minimal complications post-operation. With the application of wound Vac, patient did not experience excessive drainage from the site, and wound remained clean without purulence or necrosis. Patient immediately experienced relief from symptoms due to mass, and other than pain from surgery experienced no complications. Use of the wound Vac had not been previously documented in previous literature for wide local excision of GCT, yet was met with positive results in this specific case, and may serve for further investigation regarding recovery from wide excision of deep GCT.
Regardless of tumor malignant status, wide local excision of lesion is recommended to prevent recurrence and potential future malignant transformation. Despite this case of abnormal presentation of GCT with deep fascia and musculature involvement, wide local excision still had immediate results and improvement of patient symptoms with minimal complications. Follow up with the patient a month from the procedure showed minimal complications with failure of tumor reoccurrence. In comparison with current literature, excision of the mass appears to remain the gold standard in management of GCT. Although radiotherapy/chemotherapy was considered in this patient due to abnormal presentation, multiple nodules, and relatively deep fascia involvement, lack of malignancy and lymph node involvement pushed the decision for excision opposed to radiation. Some literature has seen some success with local steroidal treatment and silicone blocks to prevent reoccurrence and excess scar hypertrophy (Yilmaz et al. 2007). Such management was not necessary in this case due to lack of reoccurrence and no additional symptoms.
Granular cell tumor (GCT) is a rare, usually benign neoplasm. Malignancy are rare, occurring in only 0.5-2% of patients. Typical neoplastic locations are at the tongue, oral cavity, and skin with rarer types occurring at the extremities and internal organs. Generally, benign GCT has a distinct histological appearance and tends to lack skin involvement. Current literature describes benign GCT to be solitary, smaller lesions than malignant GCT. This case presents a rare occurrence with patient with multiple, painful benign GCTs with skin involvement and large size; not seen in current literature presentation.
Management with wide local excision was performed, and remains consistent with current literature as the gold standard in GCT management despite uncommon tumor presentation and appearance as shown with positive patient response to management and lack of reoccurrence.
Harvard Medical Student Review Issue 5 | January 2020